Peristomal Skin Complication Facts
Peristomal skin complications are common among people with ostomies.
The peristomal skin is the skin right around the stoma. It’s the skin that the ostomy wafer adheres to. In adults, the are of peristomal skin is approximately 4 x 4 inches around the stoma.
People with ileostomies have the most skin complications, followed by people with urostomies and colostomies respectively. Most peristomal skin complications (77%) are related to the stoma effluent (or output) coming in contact with and sitting on the skin.
Up to 80% of ostomy patients do not seek help for peristomal skin complications because they do not recognize there’s a problem. Some assume that having skin issues is “normal” with an ostomy. This is not the case! The peristomal skin should look and feel just like the rest of the skin on the person’s abdomen.
For more resources, we have a video about skin care for people with ostomies. Proper skin care is one of the most important things a person with an ostomy can do to prevent some of the complications. We also have a webinar about Troubleshooting Common Stomal Complications that cover, in detail, many of the issues mentioned below.
Please proceed with caution. Some of the photos below may be disturbing for some.
Categories of Peristomal Skin Complications
Skin complications can be identified and put into one of five categories. These categories can be remembered by the word MINDS.
M – Mechanical
I – Infection
N – Noxious chemicals and irritants (can be the person’s own effluent)
D – Diseases of the skin
S – Skin Allergens
Peristomal Skin Complications
Peristomal Skin Trauma – Mechanical

Causes: Common causes of peristomal skin trauma are pressure or friction. The most common causes of pressure or friction are
- A bad fitting appliance
- Abrasive cleaning
- Ripping the appliance off
- Frequent appliance changes
Characteristics:
- Partial to full-thickness injury
- May be painful
- Irregular borders
- Loss of skin
- Redness
Management:
- Identify what issue is causing the peristomal skin trauma. Have a WOC Nurse observe the pouching technique. They will look for rough removal, vigorous cleaning, picking, along with other common blunders that lead to this peristomal issue
Prevention:
- Patient education – cleaning, application and gentle and slow removal
- Proper fitting appliance
Treatment:
- Apply a dusting of stoma powder to the denuded (raw) skin. Let it soak in, then brush off excess. Apply the pouch right over the powder that sticks to the denuded skin
- For deeper peristomal skin trauma, like ulceration, we want to do wound care. Apply wound products and pouch right over them. Use wound products that can stay in the ulceration for a few days.
- Calcium Alginate
- Hydro-fiber
- Hydro-colloid
- Foam
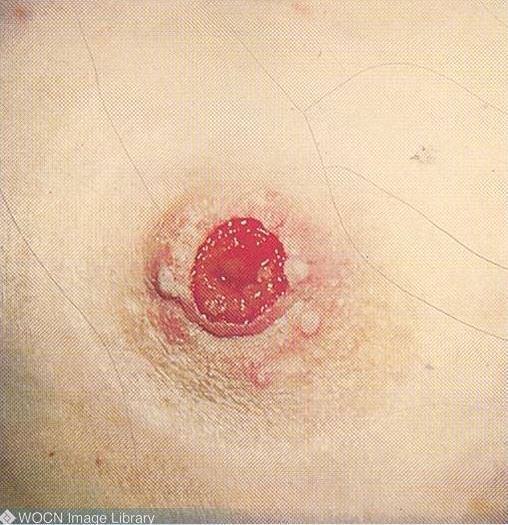
Peristomal Candidiasis – Infection (fungal)

Causes:
- Warm, moist dark areas under the skin barrier
- Can be caused by perspiration, leaks, denuded skin, prolonged wear time
Characteristics:
- Circumferential or partial rash around the stoma
- Redness and/or darker pigmentation
- Papules and pustules may be present
- Satellite lesions (scattered red areas)
- Burning or itching
- Maceration
Management
- Identify the cause of moisture (leak, climate, exercise, etc.)
Treatment:
- Candidiasis can be treated topically or, if it is a large infection or on other parts of the body, it can be treated systemically with the help of a physician
- Topically, use Nystatin powder – no creams or ointments, as they will interfere with the wafer adhering to the skin
Folliculitis – Mechanical and/or Infection

Causes: Inflammation and/or infection of superficial hair follicles
- Shaving peristomal skin too aggressively
- Ripping off the skin barrier
- Occlusion of hair follicles
Characteristics:
- Pustules or papules
- Redness
- May be painful
Management:
- Use an electric shaver and shave in the direction of hair growth
- Use adhesive remover
Treatment:
- Use antimicrobial soap to clean the peristomal skin, make sure to wash off and dry thoroughly
- Antibacterial powder
- A culture can be done to identify infection
Peristomal Contact Dermatitis – Noxious chemicals

Causes: Inflammatory reaction caused by being exposed to chemicals like the person’s own output, soap, solvents or adhesives
- Skin barrier cut too large so skin is exposed
- Skin barrier not centered
- Appliance worn too long and is breaking down
Characteristics:
- Well defined open areas of injury
- Redness
- Weeping
- Itching
- Loss of skin
- Papules may be present
Management:
- Check for any leaks (look at the back of the barrier after taking it off of the skin)
- Check to see if modification needs to be done with sizing or convexity level
Treatment:
- Clean skin with warm water (no soap)
- Apply stoma powder to weeping, injured areas and dust off excess, follow up with a barrier wipe of your choose
Hyperplasia – Noxious chemicals
Causes: Chronic exposure to urine or moisture
- Skin barrier cut too large
- High output, liquid stool or alkaline urine
- Flush or retracted stoma
Characteristics:
- Wart-like papules/nodules
- White, gray or reddish-brown discoloration
- Generally at the Mucocutaneous junction (where the skin meets the stoma)
- May be circumferential or scattered
- May bleed
- May look like crystals for people with urostomies
Management:
- Make sure you have a proper fitting pouching system
- Cover up as many lesions as possible with barrier rings or paste (without strangulating the stoma)
- For urostomates, maintain a 6.0 pH for urine by increasing fluid intake and taking Vitamin C
- For urostomates, use a pouching system with an anti-reflux valve
Treatment:
- Vinegar soaks (1/2 vinegar, 1/2 water) for about 10-15 minutes
- Sometimes the doctor may need to cauterize the hyperplasia with silver nitrate
Peristomal Pyoderma Gangrenosum (PG) – Disease

Causes: Ulcerative autoimmune disease condition
- 50% of incidence are with people who have Crohn’s Disease or Ulcerative Colitis
Characteristics:
- Painful
- Full thickness ulcers
- Begins as pustules
- The edges of the ulcers are red or purplish
- Irregular shape
Management:
- It’s imperative to manage and control the underlying disease
Treatment:
- Topical steroids and generally a physician will prescribe systemic steroids as well
- Topical anesthetic for pain
- Fill the ulcer with powder, alginate, or hydrofiber and pouch right on top of the wound products
- Never take a biopsy of this, it is diagnosed by exclusion. A biopsy can increase the problem
Peristomal Allergic Contact Dermatitis – Skin Allergens

Causes: Allergic to one or more of the products being used on the skin
Characteristics:
- Mirrored image of product person is allergic to
- Redness
- Itching
- Papules
Management:
- Perform patch test with all products used
Treatment:
- Eliminate offending product
- You can consult a dermatologist
Suture Granulomas – Mechanical

Causes: Buildup of granulation tissue at suture site
Characteristics:
- Bumps at suture site
Management:
- Consult surgeon
Treatment:
- The surgeon will decide whether to remove the sutures or not
- Sometimes a surgeon may cauterize the granulomas with silver nitrate
Peristomal Fistulas – Disease

Causes:
- Inflammatory Bowel Disease
- Improper suture placement during surgery
Characteristics: Abnormal passage between the stoma and or intestine and peristomal skin
- Effluent drains through an opening (other than the stoma) onto the peristomal skin
- The pouch won’t stay on due to fistula output and denuded skin
Management:
- Fistula pouch and hope for spontaneous closure
- Surgical reconstruction
- Stoma relocation
Most peristomal skin complications can be avoided by a properly fitting appliance. If you suspect you have any peristomal complications, please contact your doctor immediately.
All photos are courtesy of Wound, Ostomy and Continence Nurses Society. Shield HealthCare is a proud member and supporter of the WOCN Society.
For more information, see related peristomal skin articles and resources here:
- When to Contact your Doctor With Stoma Complications or Peristomal Skin Issues
- How To Clean the Skin Around the Stoma
Shield HealthCare | Medical Supplies For Care At Home Since 1957